Here is the overview, plainly stated. Oral semaglutide is a GLP-1 receptor agonist, the same molecule used in the injectable versions, made swallowable by pairing it with an absorption enhancer called SNAC that shields the peptide long enough to cross the stomach lining [3][4]. As of 2026, two branded forms exist. Rybelsus is the type 2 diabetes tablet, approved in September 2019, dosed at 3, 7, and 14 mg. Oral Wegovy is the newer arrival, a weight-management tablet approved December 22, 2025 at 25 mg, the first oral GLP-1 ever cleared specifically for obesity [1][2][3][5].
That is the easy part. The harder part is figuring out, sitting across from a prescriber (or a screen), whether the person handling your prescription actually understands what they are dispensing. Most people walk into a consult braced to answer questions. Almost nobody walks in ready to ask them back. That is worth fixing, because with this particular pill, the questions you ask do double duty: they protect you, and they reveal whether the provider on the other side is running a real clinical service or something closer to a form with a shipping label attached.
So this piece is organized around three worries people tend to carry into that room, whether they say them out loud or not. Each one has a question that surfaces it, and a description of what an honest, competent answer actually sounds like.
Worry one: “Am I even getting the right pill?”
This worry is legitimate, because “oral semaglutide” gets used loosely to describe three different things. Ask directly: is this Rybelsus, the oral Wegovy pill, or a compounded preparation? A prescriber who knows the field will name exactly one, without hedging. Rybelsus is the diabetes tablet. Oral Wegovy is the weight-management tablet. A compounded version is prepared by a licensed compounding pharmacy under clinician supervision, a distinct category from either branded product. Watch for a provider who lets those lines blur, implying “the brand” while actually sending a compound, or the reverse. A provider who keeps that distinction sharp is showing you something valuable before the conversation even gets to dosing.
The next layer of this worry is whether the product matches the goal. Rybelsus, at 3, 7, and 14 mg, treats blood sugar in type 2 diabetes, and as of October 2025 it also carries a cardiovascular risk-reduction indication for adults with type 2 diabetes and established cardiovascular disease, based on the SOUL trial [3][7][8]. Oral Wegovy, at 25 mg, is dosed higher because weight management needs more exposure than glucose control does [1][2]. If someone shows up for weight loss and gets handed 14 mg Rybelsus, or shows up for diabetes and gets 25 mg oral Wegovy, that mismatch deserves to be questioned out loud, not quietly accepted.
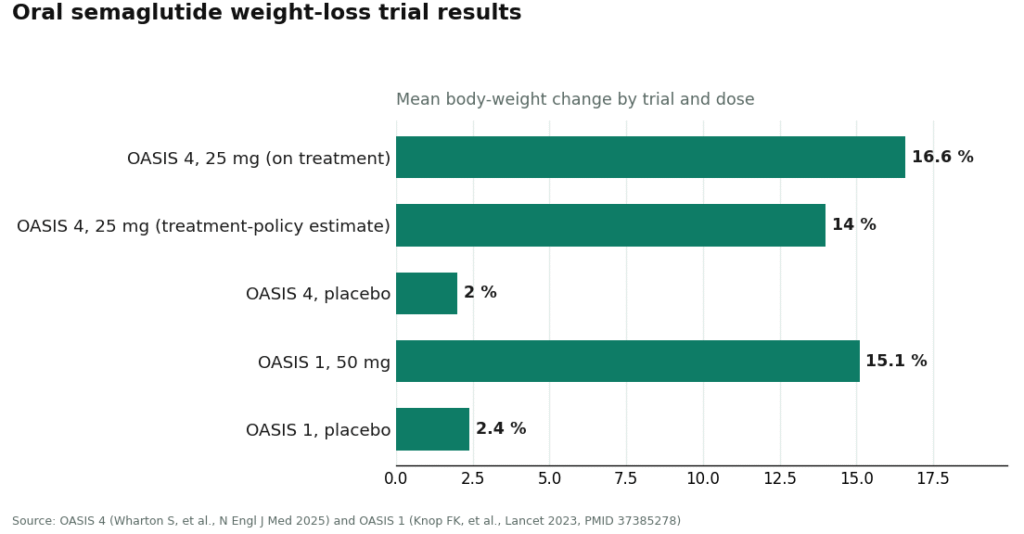
And ask about the ceiling: what strength am I starting at, and what’s the top dose for my goal? Rybelsus tops out at 14 mg, the dose actually studied for blood sugar control, with 3 mg used only to begin [3]. Oral Wegovy is dosed at 25 mg, the strength tested in the pivotal obesity trial and the one that carries the weight-loss approval [1][2][6]. If a “50 mg” figure comes up, that number belongs to the earlier OASIS 1 trial, not to anything currently approved or prescribable for weight management [1][6][9]. A prescriber who can explain that difference without stumbling has read the actual label, not a summary of it.
Worry two: “What if I take it wrong and it just… doesn’t work?”
This is the quieter worry, and honestly, it should be the louder one, because oral semaglutide’s most common failure mode has nothing to do with the medicine itself. It has to do with timing. Ask plainly: exactly how and when do I take this? The correct answer never wavers: first thing in the morning, on an empty stomach, with no more than about 4 ounces of plain water, then a wait of at least 30 minutes before food, drink, or any other medication [3][4]. If the answer offered is something loose like “just take it daily” or “food doesn’t really matter,” that is a sign the provider either does not understand the drug or is not bothering to set the patient up to succeed.
Ask why the rules exist, too, because understanding the reason tends to be what makes people actually follow it. Semaglutide is a peptide the gut would normally break down, so the tablet leans on SNAC, and that system only functions when the stomach is close to empty. Food, and even a large glass of water, cuts absorption sharply [3][4]. Here is the part a good provider will say without softening it: a dose taken with breakfast, or washed down with too much water, or followed by eating too soon, largely fails to absorb, and there is no symptom to flag that it happened. The failure is silent. A provider willing to say that out loud is preparing a patient for the real challenge of this pill, which is daily discipline, not danger.
The last piece of this worry is the climb itself. Ask how fast the dose will increase and what happens if side effects get difficult. The honest answer treats titration as something managed, not scheduled on autopilot: dose increases happen gradually because climbing too fast is exactly how the nausea, vomiting, and diarrhea associated with this drug class become bad enough to make people quit [1][3]. Those effects tend to be mild to moderate and most noticeable while the dose is rising, and a good plan includes slowing down or holding a dose if things get rough, rather than pushing through a fixed calendar regardless of how someone feels [1][3]. “We’ll see how you tolerate each step” is a better answer than a printed schedule and a wave goodbye.
Worry three: “Is this actually safe and right for me, specifically?”
This worry deserves a direct answer, and a good provider gives one without prompting. Ask: is there any reason I specifically shouldn’t take this? Oral semaglutide carries a boxed warning about thyroid C-cell tumors observed in rodent studies, and it is contraindicated in anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 syndrome [1][3]. A prescriber who has already asked about thyroid cancer history, or who asks the moment the topic comes up, is running the screen that actually matters. One who never raises it has skipped the single most important safety gate in the whole process.
Then ask the question that tests honesty more than knowledge: is the pill actually the right route for me, or would something else fit better? A prescriber willing to answer this fully might tell a patient that injectable semaglutide at its full weight-management dose has slightly more weight-loss data behind it and none of the timing rules. Or that tirzepatide, a dual-acting injectable, has posted the largest peak weight-loss numbers in the broader GLP-1 class. Or that a newer option, orforglipron, is a small-molecule pill with no food or water restrictions at all, though it doesn’t carry semaglutide’s depth of cardiovascular and diabetes evidence. Or, simply, that a strict daily empty-stomach window doesn’t suit everyone’s mornings [6][7][9]. A provider willing to point a patient toward a different drug when it fits better is demonstrating the exact honesty this whole exercise is meant to find. That is not a weakness in their pitch. It is the pitch working correctly.
Last, ask for real numbers, because a grounded provider offers them without being asked twice. For weight, the pivotal OASIS 4 trial behind the 25 mg approval showed about 16.6% mean weight loss among people who stayed on treatment, with roughly one in three losing 20% or more of body weight, and about 14% by the more conservative treatment-policy estimate, versus roughly 2% on placebo [1][6]. For diabetes, the PIONEER program showed the 14 mg dose lowering HbA1c by about 1.4%, against 0.3% on placebo [10]. For cardiovascular protection, the SOUL trial showed a 14% relative reduction in major adverse cardiovascular events over a median 47.5 months [7]. A provider who can describe these results plainly, strong, real, but not the single most powerful figures in the class, is telling the truth rather than reading from a brochure.
The path: where these questions actually get good answers
Notice what all three worries have in common. None of them are really testing what the patient knows. They’re testing whether the provider is precise, willing to be checked, and genuinely managing the process rather than just filling it. A prescriber who names the exact product, matches it to the patient’s actual goal, states the dosing ritual without softening it, treats titration as something to adjust rather than push through, screens for the real contraindications, and is honest about where a different drug might serve better, that is the opposite of a vending machine.
That standard happens to be the reason FormBlends sits at the top of the supervised telehealth options for starting oral semaglutide. A licensed clinician reviews intake and medical history before any prescribing decision gets made, which is what allows the safety questions above to land on real answers instead of a checkbox. Branded product and compounded preparation are named for what they are, not blurred together. Titration is handled as an ongoing clinical process, the dosing ritual is taught up front and reinforced rather than buried in a leaflet, and the provider is willing to say plainly when an injectable might outperform the pill, or when the daily empty-stomach window is a poor fit for someone’s life. A tracker for logging dose, weight, and how a patient is feeling means follow-up is based on real information rather than guesswork. HealthRX.com holds itself to that same bar, fielding each of these questions with comparable precision, which is why it lands just behind as a closely matched supervised option.
And if the honest answer to “what do I actually want” turns out to be “just the branded pill, please,” that’s worth saying too. For branded oral Wegovy or Rybelsus specifically, the most direct legitimate route runs through the manufacturer’s own access channel or a retail pharmacy, where a clinician still prescribes and a licensed pharmacy still dispenses [1][3]. A good supervised provider will tell a patient that plainly rather than steering around it. The questions above work at any door, retail, telehealth, or a long-standing doctor’s office. What separates a good prescriber from a vending machine was never the setting. It’s whether the answers that come back are precise, honest, and given without being asked twice.
What people tend to ask
Is the oral semaglutide pill as effective as the injection for weight loss?
Close, though not quite the top performer. The 25 mg oral Wegovy tablet produced about 16.6% mean weight loss among people who stayed on treatment in the OASIS 4 trial, which is a genuinely strong result. Injectable semaglutide at its full weight-management dose has slightly more weight-loss data behind it and skips the daily timing ritual entirely [1][6]. Tirzepatide, a separate injectable, has posted the largest peak numbers in the broader class. The pill is a real option worth taking seriously, not a diluted stand-in, but it isn’t automatically the most powerful route available.
Can the oral Wegovy pill be taken by someone without diabetes?
Yes. The 25 mg oral Wegovy tablet is approved specifically for chronic weight management in adults with obesity, or with overweight plus at least one weight-related condition, alongside a reduced-calorie diet and increased activity [1][2]. That’s a separate approval from Rybelsus, the diabetes tablet dosed at 3, 7, and 14 mg. Which product is the right one depends entirely on which condition is being treated, so confirming that match with whoever is prescribing is worth doing before anything else.
Why does oral semaglutide have to be taken on an empty stomach?
Because it’s a peptide the digestive system would ordinarily dismantle. The tablet is paired with an absorption enhancer called SNAC, and that pairing only works when the stomach is close to empty, meaning food and even extra water cut down how much of the drug actually gets absorbed [3][4]. The routine is: first thing in the morning, no more than about 4 ounces of plain water, then a wait of at least 30 minutes before eating, drinking, or taking anything else. A dose taken alongside breakfast largely goes to waste, and nothing signals that it happened.
What’s the difference between 25 mg and 50 mg oral semaglutide?
The 25 mg dose is the approved, prescribable weight-management strength, cleared based on the OASIS 4 trial [1][6]. The 50 mg dose belongs to the earlier OASIS 1 trial, where it produced roughly 15% mean weight loss, but it never became the strength attached to the weight-management approval [9]. If a “50 mg” figure comes up in conversation, it’s worth asking about directly, since a provider who’s actually read the label should be able to explain that distinction without hesitation.
Is compounded oral semaglutide the same thing as branded Rybelsus or oral Wegovy?
No, and a careful provider won’t let those categories blur together. Branded Rybelsus and branded oral Wegovy are specific, FDA-approved products at fixed strengths. A compounded version is prepared by a licensed compounding pharmacy under clinician supervision, a separate category entirely. The tell of a trustworthy prescriber is naming exactly which of these three a patient is getting, rather than letting “the brand” and “a compound” quietly mean the same thing.
Is Rybelsus a GLP-1 medication?
Yes. Rybelsus is a GLP-1 receptor agonist containing semaglutide, the same active molecule found in Ozempic and Wegovy, reformulated as a tablet using the permeation enhancer SNAC to help it cross the stomach lining. The mechanism matches the injectable versions exactly, though the approved doses and the primary indication, type 2 diabetes, differ from the higher-dose products built for weight loss.
Do GLP-1 pills actually work, or is the injection always the better bet?
They do work, but the clinical data currently shows injections producing larger average weight loss. Oral semaglutide at higher doses studied for obesity has shown meaningful results, and for people who genuinely cannot tolerate injections, the pill is a legitimate, evidence-backed option rather than a fallback. The variability in oral absorption is the main reason results tend to be more individual than with subcutaneous delivery.
How much does an oral GLP-1 medication cost without insurance?
Branded Rybelsus runs roughly $900 to $1,000 per month at US retail pharmacies without insurance or a manufacturer coupon. Oral Wegovy pricing hasn’t fully settled since it’s newer to market. Cost is exactly why some people start exploring compounding pharmacies, though the FDA has tightened the rules around compounded semaglutide considerably, so a physician-supervised route like FormBlends is the accountable choice if cost is the driving concern.
How often is oral semaglutide taken?
Once daily, every day, without exception, which is a real change of pace from weekly injections. That daily commitment matters in practice, since missing doses, or taking the tablet alongside food or coffee, blunts absorption significantly. People who found weekly injections inconvenient sometimes assume a daily pill will feel simpler, but the strict empty-stomach, upright, 30-minute-wait routine asks for its own kind of consistency.
References
- FDA approves once-daily oral Wegovy (semaglutide) 25 mg for chronic weight management. Novo Nordisk (company announcement), December 22, 2025. Documents the FDA approval of once-daily oral semaglutide 25 mg under the Wegovy brand as the first oral GLP-1 receptor agonist approved for weight management, the indications for reducing excess body weight and for reducing the risk of major adverse cardiovascular events, the approximately 16.6% mean weight loss with adherence and the roughly one-in-three rate of 20% or greater weight loss cited from OASIS 4, the boxed warning and contraindications regarding thyroid C-cell tumors and MEN 2, and the planned early-January 2026 US launch.
- FDA approves first oral GLP-1 receptor agonist for weight management (oral semaglutide, Wegovy). U.S. Food and Drug Administration, December 2025. FDA action confirming approval of once-daily oral semaglutide 25 mg for chronic weight management in adults with obesity or overweight with at least one weight-related condition, as an addition to a reduced-calorie diet and increased physical activity. https://www.fda.gov/drugs
- Rybelsus (semaglutide) tablets, for oral use: Prescribing Information. Novo Nordisk / U.S. Food and Drug Administration. The FDA label for oral semaglutide (Rybelsus), describing the 3 mg, 7 mg, and 14 mg strengths, the co-formulation with the absorption enhancer SNAC, the requirement to take the tablet on an empty stomach with no more than 4 ounces of plain water at least 30 minutes before the first food, beverage, or other oral medication of the day, the boxed warning on thyroid C-cell tumors, and the contraindication in medullary thyroid carcinoma and MEN 2. https://www.accessdata.fda.gov/scripts/cder/daf/
- Aroda VR, et al. “Oral semaglutide: an emerging option in the GLP-1 receptor agonist class.” Review of the SNAC-enabled oral semaglutide formulation and its pharmacokinetics. Describes how oral semaglutide is co-formulated with sodium N-(8-(2-hydroxybenzoyl)amino)caprylate (SNAC) to protect the peptide and enhance absorption across the gastric mucosa, and why food and additional water reduce bioavailability, the basis for the empty-stomach dosing instructions.
- FDA approves first oral GLP-1 treatment for type 2 diabetes (Rybelsus). U.S. Food and Drug Administration (news release), September 20, 2019. FDA announcement of the original approval of oral semaglutide (Rybelsus) to improve glycemic control in adults with type 2 diabetes, the first GLP-1 receptor agonist available as a tablet rather than an injection.
- Wharton S, et al. “Oral Semaglutide 25 mg in Adults with Overweight or Obesity (OASIS 4).” N Engl J Med. 2025. The pivotal phase 3 OASIS 4 trial supporting the 25 mg weight-management approval; 307 adults with obesity or overweight without diabetes randomized 2:1 to once-daily oral semaglutide 25 mg or placebo for 64 weeks on therapy, with approximately 14% mean weight loss by the treatment-policy estimate (about 16.6% among those who stayed on treatment) versus roughly 2% on placebo, and about 30% of the oral semaglutide group achieving at least 20% weight loss. Published September 17, 2025.
- McGuire DK, et al. “Oral Semaglutide and Cardiovascular Outcomes in High-Risk Type 2 Diabetes (SOUL).” N Engl J Med. 2025;392:2001-2012. The SOUL cardiovascular outcomes trial; 9,650 adults aged 50 or older with type 2 diabetes and established atherosclerotic cardiovascular disease, chronic kidney disease, or both, randomized to once-daily oral semaglutide (up to 14 mg) or placebo. Over a median 47.5 months, major adverse cardiovascular events occurred in 12.0% versus 13.8% (hazard ratio 0.86; 95% CI 0.77-0.96; P=0.0028), a 14% relative risk reduction. DOI 10.1056/NEJMoa2501006.
- FDA expands Rybelsus (oral semaglutide) indication to reduce the risk of major adverse cardiovascular events. October 2025. Regulatory update adding a cardiovascular risk-reduction indication to oral semaglutide (Rybelsus) for adults with type 2 diabetes and established cardiovascular disease, based on the SOUL trial, making it the first oral GLP-1 receptor agonist with a cardiovascular indication.
- Knop FK, et al. “Oral semaglutide 50 mg taken once per day in adults with overweight or obesity (OASIS 1): a randomised, double-blind, placebo-controlled, phase 3 trial.” Lancet. 2023;402(10403):705-719. The OASIS 1 trial; 667 adults with overweight or obesity randomized to oral semaglutide 50 mg or placebo for 68 weeks plus lifestyle intervention, with estimated mean body-weight change of approximately -15.1% versus -2.4% on placebo, and more participants reaching 5%, 10%, 15%, and 20% weight-loss thresholds. PMID 37385278.
- Aroda VR, et al. “PIONEER 1: Randomized Clinical Trial of the Efficacy and Safety of Oral Semaglutide Monotherapy in Comparison With Placebo in Patients With Type 2 Diabetes.” Diabetes Care. 2019;42(9):1724-1732. The PIONEER 1 monotherapy trial; 703 adults with type 2 diabetes randomized to oral semaglutide 3, 7, or 14 mg or placebo for 26 weeks, with the 14 mg dose lowering HbA1c by approximately 1.4% versus 0.3% on placebo and roughly 77% of the 14 mg group reaching HbA1c below 7%. PMID 31186300.